
Can we regenerate the central nervous system after injury?
- Freya Tierney
- Feb 9
- 5 min read
In the UK, an estimated 105,000 people are living with a spinal cord injury, resulting in axonal disconnection within the central nervous system (CNS) and a loss of communication between the brain and the body. This disruption can lead to profound and life-altering consequences, including paralysis, loss of sensation, and disturbances in autonomic function. Unlike peripheral nerves, which are capable of long-distance axonal regeneration and meaningful functional recovery, the CNS has a severely limited capacity to repair itself. As a result, many individuals with central neuropathies currently have no effective treatment options. Nevertheless, substantial research efforts are underway to identify therapies capable of promoting axon regeneration in the CNS, and several experimental approaches have now progressed to clinical trials, where early results appear promising.
The Science Behind Axon Growth
Axonal growth can be achieved via the stimulation of growth cones - dynamic structures found at the leading edge of axons and dendrites, involved with their development and extension. Growth cones consist of f-actin, which is the primary driver of their motility, as well as microtubules, which are found on the periphery and provide support and stability. In a resting growth cone, the microtubules ‘treadmill’: here, tubulin gets sporadically pulled into the growth cone in a process called microtubule recapture. The ‘treadmill’ can be modified in response to certain environmental cues; for example, attractant cues can slow the treadmill causing the tubulin to accumulate and grow in its direction. Alternatively, inhibitory cues can destabilise the microtubule treadmill, resulting in the collapse of the growth cone.
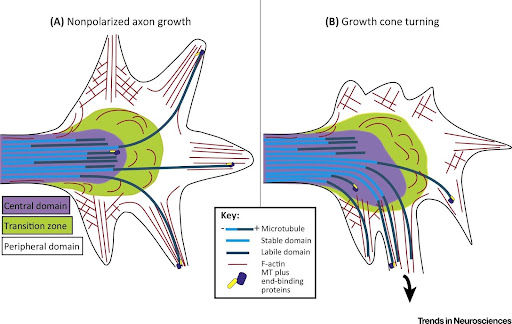
Figure 1: Structure and composition of the growth cone at rest and when turning. Growth cones consist of a central, transition, and peripheral domain, composed of f-actin and microtubules. (Kahn and Baas, 2016)
This process can be regulated through a family of proteins called GTPases, of which there are three known to regulate growth cones - RhoA, a negative regulator, and Rac and Cdc42, which are positive regulators. In particular, the enzyme RhoA is activated by growth-inhibitory factors and regulates events that result in the collapse of the growth cone, failure of axonal regeneration, and, ultimately, failure of motor and functional recovery.
What therapies have been tried so far?
Due to its central role in growth cone collapse, most research so far has focused on proteins and signalling pathways which inhibit the negative regulator, RhoA. Earlier studies explored this idea through elevating Db-cAMP levels (a cell-permeable form of cAMP). This protein phosphorylates RhoA and inhibits its activity, thus preventing growth cone collapse. Studies have found that functional recovery after Db-cAMP treatment is poor, suggesting that alone it is not enough to regenerate axons and repair the CNS after spinal cord injury.
"Interestingly, ibuprofen has also been found to inhibit RhoA via a mechanism distinct from its analgesic effects"
Alternative therapies have directly targeted RhoA and its receptor, ROCK. Molecules that directly inhibit these proteins can block RhoA signalling, thereby preventing growth cone collapse and promoting axonal growth. Molecules tested to date include C3 transferase, a RhoA inhibitor, and Y-27632, a ROCK inhibitor; unfortunately, both were demonstrated to be ineffective in living organisms. More recently, Cethrin/VX-210, a cell-permeable version of C3 transferase, showed promising results in restoring motor function in animal models and advanced to Phase 2/3 clinical trials in 2018. As of 2021, however, it was reported to be ineffective in improving motor function in humans with spinal cord injuries. Interestingly, ibuprofen has also been found to inhibit RhoA via a mechanism distinct from its analgesic effects. It was found to promote axonal sprouting and functional recovery in animal studies, however, no clinical trials to date have investigated its effectiveness in humans.
Current Research
Despite the failure of earlier trials, several ongoing clinical studies are still exploring therapies that target RhoA and its associated signalling pathways, with some showing promising early results. One such trial focuses on proteins upstream of RhoA, with the logic that inhibiting these molecules can indirectly suppress RhoA activity. Specifically, the investigated molecule is Soluble Nogo-Receptor-Fc decoy (AXER-204), a decoy Nogo receptor often referred to as a “Nogo Trap”. This protein acts by binding to and neutralising growth inhibitory factors that would otherwise activate RhoA. Because Nogo receptors normally inhibit axonal growth through RhoA activation, blocking this interaction with receptor decoys has the potential to promote axonal regeneration. AXER-204 is currently being evaluated in a Phase 2a clinical trial, with results on its safety and effectiveness in humans being awaited.
Alternatively, genetic therapies to promote axonal growth by targeting key growth-regulatory genes are being explored. The PTEN gene has emerged as a critical regulator of axonal regeneration through its inhibition of the mTOR pathway. High PTEN expression, which is typical in the adult CNS, suppresses mTOR activity, thereby limiting the intrinsic capacity of axons to regenerate. PTEN has also been shown to cross-talk with the RhoA/ROCK signalling pathway, further enhancing growth-inhibitory signalling and contributing to the suppression of axonal growth.

Figure 2: A schematic of PTEN and its relevance to RhoA/ROCK. ROCK indirectly activates PTEN, inhibiting pathways that result in axonal regeneration and neuronal survival.
Consequently, targeting PTEN is being investigated as a strategy to enhance regeneration. PTEN deletion in animal models has demonstrated significant axonal regrowth and improved motor function. Permanent deletion of PTEN is not feasible in humans due to its role as a tumour suppressor, but alternative approaches, such as PTEN inhibitors or gene therapy using RNA interference (RNAi), are being considered as potential therapies.
Conclusion
Overall, recent studies have demonstrated highly promising advances in promoting axon regeneration within the CNS. Although many earlier trials were unsuccessful, innovative strategies for targeting axonal growth pathways continue to emerge, and more are entering clinical trials than ever before. It is important to bear in mind that while achieving axonal regrowth would be a triumph, axons must still locate appropriate targets to re-establish functional neural circuits, meaning that several challenges remain to be addressed. With continued progress, however, these efforts may soon translate into viable therapies capable of transforming the lives of individuals living with spinal cord injuries.
References
This article was written by Freya Tierney and edited by Julia Dabrowska, with graphics produced by Saba Keshan. If you enjoyed this article, be the first to be notified about new posts by signing up to become a WiNUK member (top right of this page)! Interested in writing for WiNUK yourself? Contact us through the blog page and the editors will be in touch.


Comments